From “Black Box” to Moral Space
Designing a Behavioral Intervention to Increase Clinical Ethics Consultation Utilization
Zoe Lewczak, BS
About this Project
Across U.S. healthcare, clinicians encounter ethical dilemmas, yet many perceive Clinical Ethics Consultation (CEC) as a “black box”—a misunderstood resource despite its high user satisfaction. Evidence suggests that CEC remains underutilized due to a lack of awareness, procedural confusion, and skepticism regarding its practical value. To address these barriers, this capstone proposes an intervention grounded in behavioral economics, designed to guide clinicians toward ethics resources without limiting professional agency. Much like an architect designs a space to facilitate natural movement, this approach repositions CEC as a seamless, readily available support system. The intervention includes several mechanisms, such as a dedicated webpage, informational fliers, and peer-led Ethics Grand Rounds, to increase CEC visibility and reduce the navigational burden on clinicians. This normalizes CEC as a functional component of the hospital's daily flow, ensuring that ethics support is intuitive and ready when it matters most. To measure the impact of this intervention, a pilot study was designed for a non-profit, safety-net academic medical center. The study will track changes in CEC utilization and reason for consult over a 12-month period, while also evaluating ethical integrity and perceived value through a mixed-methods approach. By framing CEC underutilization as a communication challenge, this research demonstrates how a behavioral intervention can increase CEC’s utilization and evolve the perception of the ethicist from a “moral expert” to an “architect of moral space.” Ultimately, by simplifying access and humanizing ethics teams, healthcare systems can foster a culture of moral resilience, ensuring ethical complexity is no longer a solitary burden.



Think about an architect designing a physical space: they might strategically place walkways and doors to facilitate natural movement throughout a building, while avoiding the enforcement of a specific path. In the same way, a conscientious choice architect structures options to help people make decisions that align with their own best judgment.
In a similar way, a clinical ethicist is the choice architect who might provide a nudge to reduce distress; a nudge is not a command or a mandate, rather it is moral lubricant, removing the friction that prevents a clinician from acting on their best judgment.
By facilitating a family meeting or clarifying a DNR conflict, the ethicist is not making a medical decision—they are clearing the cognitive and emotional debris, so the clinician can finally see the path they already knew was right. This clearing of uncertainty ensures that the ethically appropriate path is not a hypothetical, but the most accessible route for a team under pressure.
What is a Clinical Ethicist?


Pilot Study Design
Objective: To increase Clinical Ethics Consultation (CEC) utilization by transforming the service from a “black box” into a transparent, accessible resource that enhances clinician moral resilience.
Hypothesis: If we deploy a behavioral intervention, the Clinical Ethics Consultation (CEC) utilization among clinicians will increase because there will be a better understanding of how the services works and how to access it.
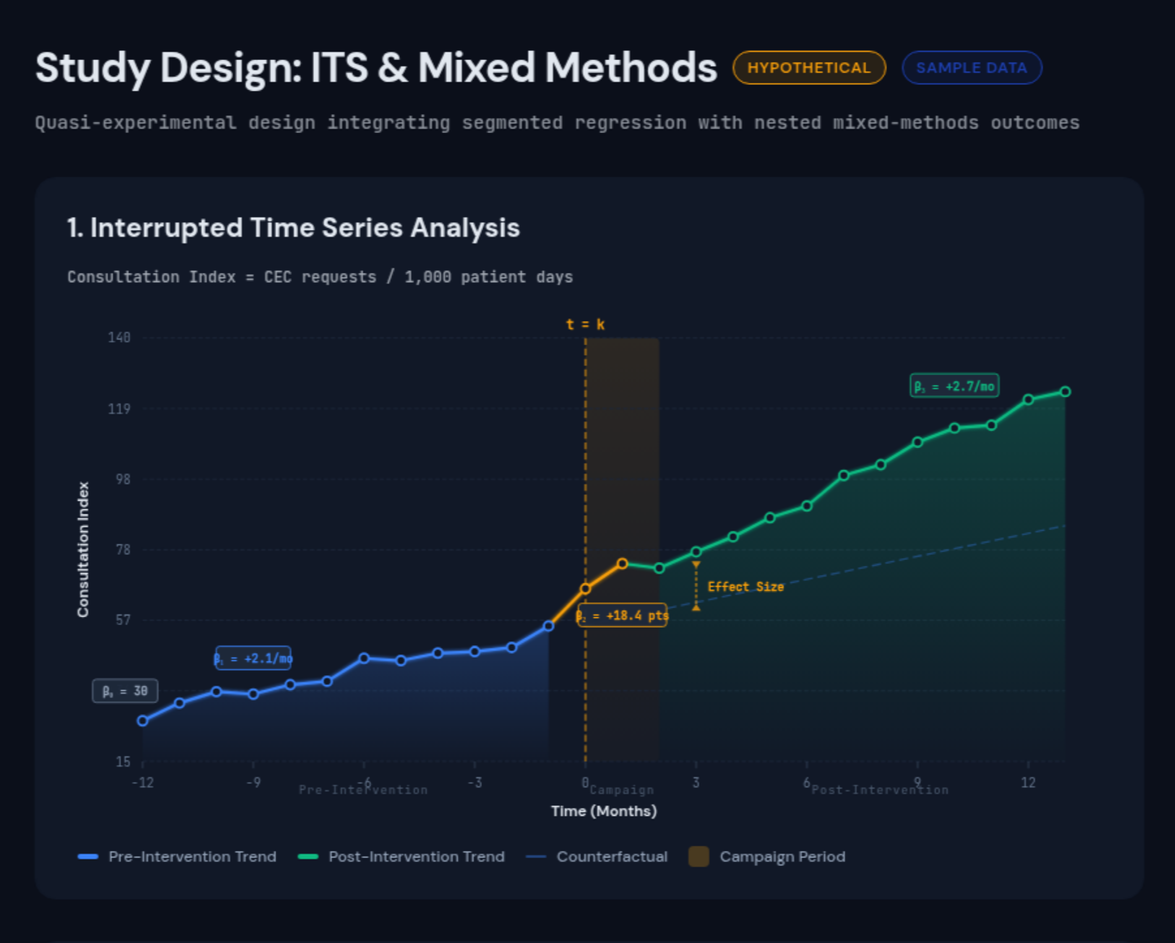
How: To capture the human impact, a Nested Mixed-Methods Cohort Study will be employed, which includes:
Baseline: The primary diagnostic tool to establish the pre-intervention state of Clinical Ethics Consultation (CEC) utilization.
Primary Outcome: Utilization Rates of Clinical Ethics Consult Services.
Tracked via the Visual Analytics Dashboard using the Consultation Index to isolate level and trend changes.
Secondary Outcome: Moral Resilience and CEC Utility.
Measured via the Rushton Moral Resilience Scale-16 (RMRS-16) integrated into the Post-Consult Follow-Up Survey (T1) to correlate increased CEC access with improvements in moral efficacy and self-stewardship.
Operationalized through the Analytic Case Evaluation for Clinical Services (ACECS) system to measure how the service was used. The Post-Consult Follow-Up Survey (T1) measures instrumental (actionable resolutions), hedonic (reduction in moral distress), and cognitive (integration into practice) benefits.
More information:
-
Click here to see manuscript draft.
-
Cederquist, L., LaBuzetta, J. N., Cachay, E., Friedman, L., Yi, C., Dibsie, L., & Zhang, Y. (2021). Identifying disincentives to ethics consultation requests among physicians, advance practice providers, and nurses: A quality improvement all staff survey at a tertiary academic medical center. BMC Medical Ethics, 22(1), 44. https://doi.org/10.1186/s12910-021-00613-7
Core Competencies for Healthcare Ethics Consultants (3rd ed.). (2025). American Society for Bioethics and Humanities.
Dubler, N. N., & Blustein, J. (2007). Credentialing Ethics Consultants: An Invitation to Collaboration. The American Journal of Bioethics, 7(2), 35–37. https://doi.org/10.1080/15265160601109366
Fox, E., Myers, S., & Pearlman, R. A. (2007). Ethics Consultation in United States Hospitals: A National Survey. The American Journal of Bioethics, 7(2), 13–25. https://doi.org/10.1080/15265160601109085
Horner, C. (2022). The Existential Crisis of Clinical Ethics Consultants. The American Journal of Bioethics, 22(4), 64–65. https://doi.org/10.1080/15265161.2022.2044560
Kaldjian, L. C., Weir, R. F., & Duffy, T. P. (2005). A clinician’s approach to clinical ethical reasoning. Journal of General Internal Medicine, 20(3), 306–311. https://doi.org/10.1111/j.1525-1497.2005.40204.x
Kelly, Christopher. A., & Sharot, T. (2021). Individual differences in information-seeking. Nature Communications, 12(1), 7062. https://doi.org/10.1038/s41467-021-27046-5
Malshe, A., Biemans, W., & Friend, S. B. (2025). Marketing strategy implementation in healthcare organizations: Navigating the challenges of marketing dispersion. Journal of Business Research, 200, 115593. https://doi.org/10.1016/j.jbusres.2025.115593
Orr, R. D., & Shelton, W. (2009). A Process and Format for Clinical Ethics Consultation. The Journal of Clinical Ethics, 20(1), 79–89. https://doi.org/10.1086/JCE200920112
Rushton, C. H. (2023). Transforming Moral Suffering by Cultivating Moral Resilience and Ethical Practice. American Journal of Critical Care, 32(4), 238–248. https://doi.org/10.4037/ajcc2023207
Rushton, C. H., Hanson, G. C., Boyce, D., Holtz, H., Nelson, K. E., Spilg, E. G., & Robillard, R. (2024). Reliability and validity of the revised Rushton Moral Resilience Scale for healthcare workers. Journal of Advanced Nursing, 80(3), 1177–1187. https://doi.org/10.1111/jan.15873
Seeking and Giving Consultation. (2007). The American College of Obstetricians and Gynecologists.
Sunstein, C. (2020). How Fun Might Move the World. The Decision Lab. https://thedecisionlab.com/podcasts/how-fun-might-move-the-world
Sunstein, C. R. (2014). Nudging: A Very Short Guide. Journal of Consumer Policy, 37(4), 583–588. https://doi.org/10.1007/s10603-014-9273-1
Sunstein, C. R. (2021). The Feast Framework For Behavior Change.
Tapper, E. B. (2013). Consults for Conflict: The History of Ethics Consultation. Baylor University Medical Center Proceedings, 26(4), 417–422. https://doi.org/10.1080/08998280.2013.11929025
Tarzian, A. J. & Asbh Core Competencies Update Task. (2013). Health Care Ethics Consultation: An Update on Core Competencies and Emerging Standards from the American Society for Bioethics and Humanities’ Core Competencies Update Task Force. The American Journal of Bioethics, 13(2), 3–13. https://doi.org/10.1080/15265161.2012.750388
Thaler, R. H. (2018). Nudge, not sludge. Science, 361(6401), 431–431. https://doi.org/10.1126/science.aau9241
Walker, M. U. (1993). Keeping Moral Space Open New Images of Ethics Consulting. The Hastings Center Report, 23(2), 33. https://doi.org/10.2307/3562818
Zajonc, R. B. (1968). Attitudinal effects of mere exposure. Journal of Personality and Social Psychology, 9(2, Pt.2), 1–27. https://doi.org/10.1037/h0025848
Acknowledgements
Special thanks to Michael Ieong, MD, HEC-C and Casey Rojas, JD, MBE, for their invaluable mentorship and guidance throughout the development of this project. And a special thanks to the Harvard Medical School Center for Bioethics faculty and peers for their feedback and support throughout this past year. Finally, thank you to Boston Medical Center’s Ethics Team for their support of this project and commitment to ethical practice.